
‘And yet, you try’
A father's quest to save his son

A speedboat cut across Lake Tahoe on a sunny day in October 2012.
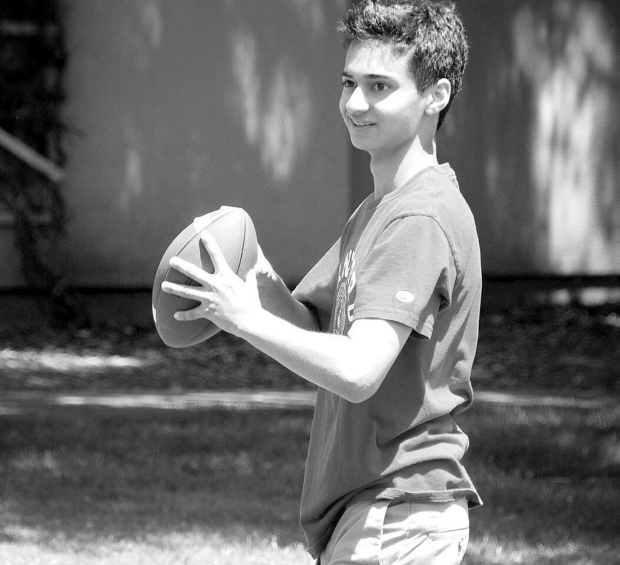
With two of his closest friends at his side, 14-year-old Milan Gambhir rode an inflated raft tethered to the back of the boat. The boys bounded over each wave, laughing as the water splashed back over them. “Half the fun was falling off into the cool water,” Milan’s friend Christopher “Kiki” Fann remembers. But the boat was going so fast that when Milan lost his grip on the raft’s handle, his head hit the water hard. “He just went flying,” Fann says. Instead of cushioning Milan’s landing, the water hit him like a wall.
“When he got back in the boat we were asking him questions, trying to tell if he was OK or not,” says Fann. “He had trouble with some of them, which was disconcerting, because a guy who was as smart and bright as he was suddenly couldn’t say the alphabet backwards.” Also on the boat was Fann’s mother, a physician, who determined that Milan had a slight concussion. She drove him to the local emergency room. There, doctors suggested a CT scan — a method of imaging that combines multiple X-rays to produce a single three-dimensional image of the inside of the body. She telephoned Milan’s parents at home in Portola Valley to get their permission for the scan.
Milan’s father, Sanjiv Gambhir, MD, PhD, who goes by the name Sam, is also a physician, an expert in diagnostic imaging who chairs the Stanford Department of Radiology and also directs Stanford’s Molecular Imaging Program. He and Milan’s mother, Aruna Gambhir, CEO of a small San Francisco biotechnology startup, agreed that the scan was necessary to make sure their only child didn’t have a hidden brain bleed or skull injury. “Let’s play it safe,” Sam Gambhir recalls thinking.
Milan’s CT scan was clear. His father and Milan’s aunt, Sangeeta Gambhir, MD, a radiologist in San Francisco, scrutinized the image later and saw that not only was there no injury or bleed, there were no problems of any kind. Milan’s brain looked healthy.
But beneath Milan’s apparent vitality was a vulnerability he’d carried since conception, one so microscopic that a CT scan could not detect it. Perhaps radiation from the CT scan itself set in motion cellular changes that were the beginning of something much worse than a concussion. A tumor was developing in Milan’s brain, one so aggressive that even his father — a renowned expert in early cancer detection — could neither anticipate nor defeat it. Nine months later, the CT scan Milan had in Tahoe had become a time stamp, marking the last confirmed date his brain was seemingly healthy.
Back at home, Milan continued immersing himself in his freshman year at Bellarmine Preparatory School in San Jose. He participated in speech and debate, jazz band and twice-a-week hapkido martial art classes, where he was on track to earn his black belt. Already a piano player and percussionist, Milan had taught himself to play guitar in middle school from YouTube tutorials, becoming skilled enough to teach other kids.
“Each day at lunch and break time he’d jam in the band room with me and our friend Jose,” says Fann. “He’d show us chords, notes, riffs and stuff.” On weekends Milan would have friends over for video games, pool parties and some Airsoft rifle target practice, which left a speckling of telltale pockmarks on the metal rim of the chimney far above the pool.
The preceding summer, Milan had worked alongside his father in the Canary Center at Stanford for Early Cancer Detection, where Sam Gambhir is the director. In 2011, Gambhir had received a five-year, $10 million grant from the Ben and Catherine Ivy Foundation to use molecular imaging to improve the detection and management of one of the deadliest brain tumors, glioblastoma multiforme. “Milan was learning about basic techniques in keeping a lab notebook, how chemical solutions are made, that sort of thing,” says Sam Gambhir. Laboratory regulations prevented Milan from working with any cell specimens, but he was still excited to be there.
Milan’s experience in his father’s lab helped pave the way, midway through his freshman year, for a position in the research lab of Adam de la Zerda, PhD, assistant professor of structural biology and of electrical engineering at Stanford.
De la Zerda accepts only about one in a hundred high school students who apply to work in his lab. “Most of them want the recommendation letter for college, and their parents are pushing them,” he explains. “But once they get to the lab they couldn’t care less about research. They hate it. They’d much rather spend their time outside playing soccer.” Milan was happy to do both.
His first assignment was a statistical simulation of how photons proliferate in the human body. “Now, in order to do a really good job there, you need to know calculus, which of course being a 14-year-old kid he did not know at the time,” de la Zerda would say later. “So there I found myself explaining to him what integrals and double integrals are. Then Milan looks at me and asks, ‘But wait — we live in a three-dimensional space, so we probably would want to know how many photons we have in a full volume.’ So I asked him, ‘How would you calculate it?’ And there he was; he jumped at my whiteboard and started writing triple integrals on it, as though it just came to him intuitively.”
Milan worked on the project for about five months. When summer came, he started driving to work with his father and working full time in de la Zerda’s lab. In mid-July 2013, Milan came to de la Zerda with a new idea.
Milan explained: His mother had recovered from two instances of breast cancer — the first when Milan was a year old and she was 37, then again 10 years later — and her father, Milan’s grandfather, had died from esophageal cancer in his 50s. As a cancer survivor, Aruna was advised to return for frequent check-ups. To make life easier for survivors like his mom, Milan wanted to develop a comfortable, low-cost ultrasonic wristband device that could diagnose a recurrence of cancer through microbubbles that would attach to circulating tumor cells in the bloodstream.
He took de la Zerda through his plan: “He was talking about using antibodies to detect circulating tumor cells. He was going to use this small ultrasound device, and had been looking at several companies that sell them. He was convinced there was one that could be miniaturized. He had a really good plan.”
“Milan was always up early, excited about going to work,” Aruna Gambhir says. “I never had to wake him.” But just two days after he’d told de la Zerda about his idea, and only a few days before his 15th birthday, Aruna had trouble getting him up. “It was very unusual,” she says. Later that morning, walking through the parking lot with his father, he dropped his mug. His father didn’t think much of it — people drop things all the time — until later that evening. Aruna was home with Milan, eating dinner and watching television, when Milan suddenly started talking gibberish. “I said, ‘Stop it, Milan,’ ” Aruna recalls. “But he kept going, and spilled his milk. A minute or two later, when it stopped, I asked him what was going on.”
“I couldn’t control it,” Milan told her. “I don’t know what’s going on.”
Milan’s parents drove him to the Stanford Health Care emergency department. On the way in, Sam Gambhir called his colleague Shreyas Vasanawala, MD, PhD, associate professor of pediatric radiology, who met them there.
“There was a concern that he might be having a stroke,” Vasanawala says. “We started with a CT scan, which showed that Milan had some bleeding in his brain. From that, Sam already knew there was a serious situation. The next step was to try to get a better understanding of what might be causing the bleeding. For that, we did an MRI.”
“It was probably 3 in the morning when we got the diagnosis,” Aruna says. “Sanjiv saw the scan as it was coming out.”
He and Aruna, side by side with Milan, took in the news and did their best to remain calm. ‘I actually don’t know how they did it.’
Doctors confirmed what Milan’s father could already see: Milan had a brain tumor measuring about 2½ inches. Worse, the tumor was likely a glioblastoma multiforme, the very tumor Sam Gambhir had been investigating in his lab. Gambhir knew GBM all too well. A type of glioma tumor, arising from the brain’s glia cells, GBM is one of the most aggressive cancers, commonly taking the lives of patients just 14 months after diagnosis. Fewer than 5 percent survive for more than five years. For Gambhir, the coincidence was brutal.
He and Aruna, side by side with Milan, took in the news and did their best to remain calm. “I actually don’t know how they did it,” says Vasanawala. “They must have wanted to do that for Milan, too. And even Milan, over the entire course of things, was an exceptionally composed and mature person. I still don’t understand how somebody that young could be so aware and mature.”
“It was good that I didn’t know what lay ahead. I was clueless,” Aruna says. “My beautiful son. The worst thing he ever had in his life before then was a cold. One time he had the flu, maybe a knee scrape but nothing beyond these tiny little things. Nothing at all. I said, it has to be an infection or something. It cannot be this. Not the worst-case scenario.”
Aruna pinned her hopes on her husband. “We have Sanjiv here, and he can get us access to everything,” she remembers thinking. “We’re going to be fine. ‘Don’t worry, Milan. Everything’s going to be OK.’ But Sanjiv knew. That was the problem, that he knew. Sanjiv was the one who needed to be sedated.”
Sam Gambhir’s role as a specialist at Stanford Medicine, his work on GBM and his access to a worldwide network of medical experts were all sources of hope for his family. Yet that hope eluded Gambhir himself.
“From the very beginning, based on what I knew about this particular disease, I knew the chances of beating it were so small, especially because by the time Milan’s GBM was caught it was already quite spread,” recalls Gambhir. “It is more frustrating and anxiety-provoking when you know what the outcomes of patients with GBM are. And you feel helpless to do anything. And yet, you try.”
Immediately, he began communicating with colleagues at Stanford and beyond. One of his first calls was to Parag Mallick, PhD, assistant professor of radiology at Stanford and director of a lab within the Canary Center that focuses on precision diagnostics. Mallick had been personally recruited to the Canary Center in 2011 by Gambhir, who trusted his expertise in the study of therapeutic response, and in predicting which drug is likely to work on which patient.
‘I think it was the first time in his life that science disappointed him. You commit your life and work to science, and then, it’s almost like religion: How could you fail me now?’
Mallick was home when he received Gambhir’s call. “He started off very rational,” Mallick recalls. “He said, ‘I hope I’m not bothering you.’ I said, ‘No, what’s up?’ ”
Gambhir relayed the details of Milan’s diagnosis, and was soon speaking through tears. “He was trying to figure out what we had to do from day one to make sure that we gave Milan the best chance, and asking if I could help.”
“We have to save him,” Gambhir said.
“He knew that molecular analysis would be important,” says Mallick, referring to the process of profiling the tumor’s DNA, RNA and protein. “So he wanted to know what we could do, what we should do. He also recognized that he wasn’t in a state to drive the process himself — he was, understandably, hugely emotional and needed to focus on being with his family. At the same time, he knew the surgery would be happening soon, and that the resected tumor tissue needed to be handled in a way that could be scientifically and clinically actionable — that it must be saved, and saved in the right way. Because you only have one shot. If you don’t collect it right and store it right, there is no hope for precision medicine.”
Precision medicine — care tailored to a patient’s unique molecular profile — is the vanguard of cancer treatment. Specific molecular markers of an individual’s tumor cells can be used to identify the most beneficial therapeutic approaches. To obtain a reliable genome sequence of Milan’s DNA, to develop testable cell models and to enroll Milan in clinical trials all depended on his tumor tissue being carefully resected and handled properly. “There was a lot of frenzied planning prior to the surgery,” says Mallick. “All in just a few days.”
Another concern was removing as much of Milan’s tumor as possible without harming his brain. “Even though you do surgery,” says Sam Gambhir, “there’s just no way to catch the cells that have already spread to other parts of the brain. And you know those will be the ones that will eventually come back and lead to death.”
The morning after his son’s diagnosis, Sam Gambhir, who still hadn’t slept, stopped by to see Milan’s oncologist, Paul Fisher, MD, chief of the division of child neurology. “He came into my office and just cried for about half an hour,” Fisher says. Fisher, who has two decades of experience treating patients with brain cancers including glioblastoma, could offer little hope. Even the most advanced treatments ultimately fail against GBM. “Sam was taken aback by this chasm between the scientific — the basic-science world — and the clinical world, what we’re able to do for patients. I think it was the first time in his life that science disappointed him. You commit your life and work to science, and then, it’s almost like religion: How could you fail me now?”
But Gambhir was still determined to do whatever he could. “Sam obviously wanted progress for Milan’s sake,” Fisher says, “but he also knew that any progress that helped his son would also be for the greater good.”
Milan spent a few days in the hospital following his diagnosis, and was then given clearance to celebrate his 15th birthday at home. “A bunch of his friends came over,” says Aruna Gambhir. “Everyone knew something was wrong and he was going to have a surgery the following Monday. But at least we had him home for the weekend.”

Surgeon Michael Edwards, MD, professor of pediatric neurosurgery at Lucile Packard Children’s Hospital Stanford, led the surgery on July 22 to remove Milan’s frontal lobe mass, sending the resected tissue to neuropathology where sections could be made to release for research. From there, Milan’s cancer cells were personally handled by Michelle Monje, MD, PhD, an assistant professor of neurology at Stanford who was the first to culture brainstem glioma cells from a deadly childhood tumor called diffuse intrinsic pontine glioma. Monje carefully cultured Milan’s cancer cells so they could be grown, de-identified, and distributed worldwide for research.
“These types of cell cultures are rare,” says Monje. “Few labs successfully make these cultures, and even fewer distribute them widely for use. Yet they’re very important for understanding the fundamental biology of these tumors and developing more effective therapies.”
Monje and her team sent Milan’s de-identified cultures to about 30 research labs around the world, as well as several labs right on the Stanford campus. “His cells are now in every country that does high-impact research on pediatric high-grade gliomas,” she says. “In Canada, Spain, England, China, all over the world.”
Three days after Milan’s surgery, Sam Gambhir emailed James Ford, MD, professor of oncology and of genetics and director of the Stanford Clinical Cancer Genetics Program. He asked Ford about the likelihood of genetic or hereditary conditions playing a role in his son’s glioblastoma diagnosis. “We talked about his wife’s history of breast cancer,” Ford says. “Her father also had cancer, and now her son had contracted glioblastoma at a young age. I suggested we start by testing for Li-Fraumeni syndrome.”
Li-Fraumeni syndrome — named for Frederick Pei Li and Joseph F. Fraumeni Jr., the American physicians who first identified it in 1969 — is a rare, inherited condition that dramatically increases the risk of many types of cancer. Since 1969, approximately 500 families worldwide have been reported to have the condition, though its actual prevalence is unknown. In his discussion with Gambhir, Ford heard the indicators that tipped him off: a family with multiple generations of cancer diagnoses, including childhood brain cancer and breast cancer in a young woman.
Most patients with Li-Fraumeni are more susceptible to cancers because of a mutation in what Ford calls the most important gene in all cancers: the gene for tumor protein 53, or p53. When it’s functioning properly, p53 is indispensable, playing several roles, including supervising our cells’ growth and DNA replication and, when DNA is damaged, activating repair proteins. If the cell fails to repair, p53 can either halt the cell’s growth or initiate its death. DNA damage is commonly caused by things like overexposure to sunlight or other forms of radiation, smoking, toxins in food or pesticides, or simply from aging and normal metabolism, but if that damage doesn’t develop into cancer, it’s because p53 is on the job.
Most patients with Li-Fraumeni syndrome have inherited a mutation in the p53 gene that prevents it from performing its lifesaving role in routine DNA repair. As a result, cells with damaged DNA grow freely, resulting in additional genetic mutations and allowing a variety of cancers to proliferate, particularly sarcomas and cancers of the breast, brain and adrenal glands. These account for about 80 percent of all cancers in patients with Li-Fraumeni, many of which are treatable when caught early. Lifetime cancer risk for men with the syndrome is up to 85 percent, and nearly 100 percent for women, largely due to the increased likelihood of breast cancer.
“It’s very different than, for example, inherited BRCA1 or 2 gene mutations that increase a woman’s risk for breast and ovarian cancer,” says Ford. “Those are bad enough, but at least you know what tissues to focus screening on. In Li-Fraumeni syndrome, you’re at risk for cancer anywhere in the body.”
‘With my dad dying, and then me getting it, and then Milan getting sick, there was some reason for it. But there was no relief. Milan got the worst of the worst cancer he could have gotten.’
Most people haven’t heard of Li-Fraumeni syndrome, because so few people are diagnosed with it. “At Stanford, our genetic counselors and our clinic saw over 1,500 patients last year for genetic counseling and genetic testing for cancer families,” Ford explains. “Of those, maybe 10 were considered for Li-Fraumeni.” Even this, he says, is a big increase from five to 10 years ago: “With more comprehensive genetic testing, we’re finding these families more often.”
About a week after his glioblastoma diagnosis, and after genetic counseling, Milan was tested for Li-Fraumeni syndrome. A few weeks later, so was his mother. Both tested positive for the inherited p53 mutation.
The Li-Fraumeni diagnosis helped Aruna Gambhir understand her family medical history. “I could say, ‘Oh, I see. That’s what’s been wrong,’ ” she recalls. “With my dad dying, and then me getting it, and then Milan getting sick, there was some reason for it. But there was no relief. Milan got the worst of the worst cancer he could have gotten.”
The deeper diagnosis of Li-Fraumeni also helped Milan’s parents understand how their son could be diagnosed with an advanced brain tumor just nine months after having had a clear CT scan. “It’s possible that he developed this tumor from the CT scan radiation,” says Sam Gambhir. “When you carry this p53 mutation, you are much more susceptible to radiation. In a normal person, a CT scan wouldn’t be a big deal. But in someone with this mutation, it likely increases their chances of cancer. We will never know for sure.”
For those who know they have Li-Fraumeni syndrome, regular monitoring is crucial to detect cancer early and at a potentially curable stage. But because of patients’ heightened vulnerability to radiation exposure, the method of diagnostic monitoring is just as important as the frequency. Ford and his team use only annual whole-body MRI scans. Magnetic resonance imaging uses strong magnetic fields and radio waves to create images, making it a safer option than CT scans and X-rays.
“If you know the risk, and know which cancers you’re at risk for, and at what age, often you can detect them early enough where you can deal with them and often cure them,” says Ford. And that is the painful irony of Milan’s diagnosis, he adds, “because of course Sam’s entire career is focused on this, and that’s what the Canary Center is dedicated to.”Sam Gambhir’s lab and other labs in the Canary Center at Stanford are making advances in early detection of a variety of cancers, from blood-based “in vitro” diagnostics that sample blood, urine, stool, saliva, tears or breath to newly identified biomarkers — molecules that are early, telltale signs of illness — as well as devices that can spot them.
“We’ve been developing newer imaging techniques like photoacoustics where light goes into your body, interacts with the tumor and then produces sound that we can detect. Light in, sound out,” Gambhir says. “And radio-frequency acoustics, where we send radio-frequency waves in, they interact with the tumor, and send sound out.” Stanford physicians performed the world’s first prostate cancer imaging with photoacoustics in 2015. And the Gambhir lab is preparing to test devices that conduct imaging while people are going about their regular lives: a “smart bra” that continuously images breast tissue and a “smart toilet” that looks for molecules in stool and urine that could be biomarkers of colorectal cancer or prostate cancer.
“We think the best populations to test these on first are high-risk for the disease, and Li-Fraumeni is one of those,” says Gambhir. “Also patients who already have the disease, in whom we’re looking for recurrence.” These methods show promise for early detection of a variety of cancers, but glioblastoma multiforme is not one of them. “It’s more difficult because it’s a rare tumor, so it’s harder to get blood samples from patients. But also because of the blood-brain barrier. Things that are being shed by the tumor in the brain aren’t necessarily available in the blood or urine. So it’s important to understand that glioblastoma is likely one of the last tumors we would try to do early detection for. It’s just not a tractable problem right now.”
Ford emphasizes the importance of counseling Li-Fraumeni patients and families on the stress of living with their heightened cancer risk, as well as helping growing families understand their reproductive options. When one parent has Li-Fraumeni syndrome, choosing to adopt children is one way to avoid the 50 percent possibility of passing the gene on to their child. Other families opt for in vitro fertilization so they can select embryos that do not contain the mutation. When genetic test results confirm Li-Fraumeni in the midst of a pregnancy, some parents choose to terminate.
“It raises all kinds of interesting paradoxes about what you do with genetic mutations like this that aren’t lethal at the time you’re born, but carry a bad prognosis,” says Sam Gambhir. “Some family members have lived almost to the age of 60. It’s very uncertain. If we had known this diagnosis before Milan was born, would we have chosen to abort? If so, he would have never existed, and then we would never have had the 16 years we did have with him. Even having those 16 years is better than having no years.”

Since the day of Milan’s diagnosis, Sam Gambhir had been “madly searching, literally working around the clock trying to find something that could slow down this tumor,” he says.
“Sam was emotionally overwhelmed for a while,” recalls Mallick. “He was still effective and reaching out across the globe to get answers, but you definitely felt this sense of helplessness and desperation — something you never feel from Sam.” But then, one day, he just snapped out of it. “I remember him saying to me something along the lines of, ‘I feel more awake, aware, plugged in and on top of things than I have ever in my career.’ And so there was this radical transformation where he went from being in shock and dismay to taking charge. It was remarkable, seeing him click back over into problem-solving scientist mode.”
Gambhir’s widespread search led him to explore some unorthodox therapeutics. At a medical conference a few months after Milan’s diagnosis, Gambhir noticed a poster identifying a natural plant extract as a potential anti-cancer agent. The plant, called ashwaganda, had been known for thousands of years in Ayurveda medicine — a natural healing system originating in India about 5,000 years ago — to have some unusual properties against many diseases. “I said, well, this is a long shot, but why don’t we test it?’ ” Gambhir says.
After his surgery, Milan had radiation therapy for about seven weeks, which was necessary to keep his tumor in check, even though it might also cause further cell damage. “He had braces,” says Aruna Gambhir, “and had to go to the orthodontist to get them removed so that they could do the radiation therapy.” For analysis of Milan’s image findings and guidance on his therapy, Sam Gambhir relied on his colleagues Sarah Donaldson, MD, professor of radiation oncology, and professors of radiology Nancy Fischbein, MD, and Tarik Massoud, MD, PhD.
Milan was well enough to return to school for his sophomore year, and the family did its best to return to a sense of normalcy. Even before he went back to school, Milan was determined to keep up with the activities he’d started before he got sick. “Not only did he continue working in the lab,” says Aruna, “but he was doing an accelerated precalculus class so that he would qualify to take advanced-placement calculus when he went back to school in the fall as a sophomore. We told him to take a few months off or reduce his load, because he was in all honors and AP classes. But the only thing he would drop was speech and debate, which was hard for him to give up. He was full-on, full throttle. That’s the kind of kid he was.”
“Most people, if they were as sick as Milan, would take a break, go to the beach, relax,” says de la Zerda. “How many people would say they want to push even harder to focus even more on their work? Milan never let go. He had the utmost dedication and passion you can imagine.”
“I think how he saw it,” says Fann, “was that it was this physical thing he had to overcome, and that he could do it with hard work like he had always done.”
From October 2013 through May 2014, while undergoing several courses of chemotherapy and cancer vaccines, Milan presented his diagnostic device concept at five different science competitions. He was named a regional finalist at the Siemens Competition, a grand prize winner at the 2014 Synopsys Silicon Valley Science and Technology Championship and a Fourth Grand Award winner in Medicine and Health Sciences at the Intel International Science and Engineering Fair in May. To the first competition, he wore a hat to cover the areas where his hair had not yet grown back. “Milan never let anybody in the competitions know about his situation,” says Aruna. “He wanted to win purely by his own merit.”
Aruna Gambhir also had to attend to her own health. After her recurrence of breast cancer when she was 47, doctors had advised her to eventually undergo, a complete hysterectomy — surgical removal of the uterus and cervix — based on the increased risk of uterine cancer in women with certain types of breast cancer. “At that point I thought, let me just wait on that,” she says. “I wasn’t ready.” But her Li-Fraumeni diagnosis introduced a new urgency, and Aruna had the preventive hysterectomy in the summer of 2014. “I didn’t want something to happen where I couldn’t support Milan,” she says. “I just had to get it over with so I could get home and focus on him.”
That summer, Milan continued to work in de la Zerda’s lab, celebrated his 16th birthday and earned his driver’s license. On Sept. 1, 2014, he drove himself to his first day of his junior year at Bellarmine. “I guess he is not that sweet baby who held on to my hand before the start of preschool,” his mother wrote on the CaringBridge web journal that she used to keep friends and family updated about his life. “Milan is cherishing his independence.”
“We didn’t really talk about how sick he was, or how he felt about it,” Fann says. “We spent a lot of time driving his car around, playing music, just trying to be normal.”
Just a couple of months later, in November 2014, an MRI scan revealed a new tumor at the base of Milan’s skull. “When we got the news of the recurrence, he went into his room for a few minutes,” Aruna Gambhir says. “Then he came out and said he was ready to fight.” Milan had a second surgery to remove the new tumor, followed by radiation treatments that lasted until January 2015. In February he went to Gainesville, Florida, for six weeks to undergo an experimental stem cell transplant designed to manipulate his cells to mobilize his immune system. “It was a clinical trial of one,” says Aruna Gambhir.
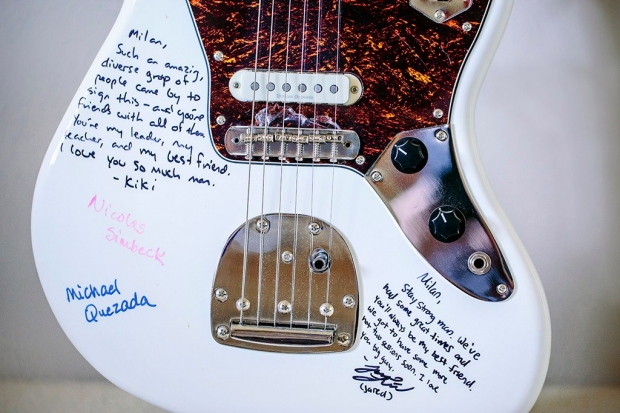
His friends all pitched in to buy Milan a white electric guitar, which they signed with messages of hope and affection. Jose Hernandez, the friend Milan and Kiki Fann had played guitar with in middle school, rode his skateboard more than 9 miles from his home in East Palo Alto to sign the guitar and help present it to Milan. “He was the best teacher I ever had,” Hernandez told Aruna Gambhir.
After a year and a half of study, Sam Gambhir and his team confirmed that a molecule in the ashwaganda plant known as Withaferin A was indeed an active ingredient with significant anti-brain-tumor effects. Best of all, since the drug was a natural agent, it would require neither FDA approval nor a prescription to administer to patients. The results were published as the cover story in the January 2016 issue of the Journal of Neuro-Oncology.
For Milan, the results came too late. “We saw that it was working in the last few weeks before he died,” Gambhir says. “But I had worries that it might cause some unexpected toxicity.” Milan was too ill to undertake a new treatment, even a natural extract. “His death was extremely hard, because he lost his hearing, then he lost his vision, then he lost his ability to speak, his ability to move, and he was in home hospice for several months.” On May 2, 2015, 21 months after his tumor was diagnosed, Milan died. He was 16 years old.
Milan’s laptop still sits on his desk in the home office he shared with his mother. Its cover bears the cardinal “S” for Stanford, where he had always hoped to enroll as a freshman this fall. Instead, a memorial for him was held on May 13, 2015, in Stanford’s Memorial Church. The grand Romanesque Revival sanctuary, which seats 1,200, was nearly full. Two family friends performed “Tears in Heaven,” by Eric Clapton, on the guitar, and a recording of one of Milan and Kiki Fann’s jam sessions was played. Carolyn Carhart Quezada, the mother of one of Milan’s closest friends since preschool, remembered Milan building his own lemonade stand out of PVC pipe, and later helping her son build a computer. She called him “a friend of a lifetime.”
“I keep hearing that he’s gone,” says Fann, “but I just feel like he’s still here and still helps me through things. I think, if Milan were here, how he’d encourage me to do things differently. And that’s made me try things I might not have tried, like speaking out in speeches and classes. And I’m still playing guitar, working on an album this year, and planning to major in music at college.”
Milan lives on not only through the memories of his family and friends, but through his scientific legacy. Today, as glioblastoma research progresses in labs around the world, his living cells, coded in anonymity, are part of it. And a few days after Milan’s death, the Wearable Ultrasonic Device for the Early Detection of Tumor Recurrence he had developed with de la Zerda was granted its patent. Sam Gambhir’s lab will oversee the process of bringing a device to fruition, which is expected to take several years. Lab members are also preparing the related research paper, which Milan kept working on until the final stages of his illness, for publication. “We’re hoping it will come out sometime soon,” says de la Zerda. “And when it does, I have all expectations that it will draw a lot of attention.”
For Sam and Aruna Gambhir, grief is woven into the fabric of their lives now. “The worst has already happened,” Aruna says. “We can’t change it.” Though Aruna must continue to monitor her own cancer vulnerability, finding the motivation to do so is, for the moment, difficult. “I don’t want to go in there,” she says, referring to the cancer clinic. “I’m not sure when I’ll want to.”
“I have a tough time walking through Lucile Packard Children’s Hospital now,” Sam Gambhir says. But the experience also deepened his empathy for other parents. “I think I was always empathetic toward illness,” he says, “but not as empathetic as I am now, knowing what it’s like to have a sick child.”
Around the time Milan had his second surgery, “I remember seeing a parent in the hospital with a small baby who had a brain tumor,” Gambhir says. “It was so good to be able to try to talk to them and comfort them. It also made me appreciate how lucky we were that Milan made it to 16 years.”
