
Hearing things
Patients were bothered by the sounds of their eyeballs, their digestive systems, their blood. One look in their eyes, and a surgeon-scientist knew why

In the spring of 1995, a patient with a bizarre set of symptoms entered the office of Lloyd Minor, MD, an expert on inner-ear disorders at Johns Hopkins.
The 50-year-old gentleman told Minor that when he sang in the shower, the items in the shower — the shampoo bottle, the loofah, the shower head — began to move about. And it was always in a specific pattern, as if the items were following one another around the face of a clock. The patient told the doctor that he had also noticed that if he hummed a similar tone or heard certain loud noises while looking in the mirror, he saw his eyes move in response.
“And in fact he said, ‘Look, I can show you,’ ” says Minor, now dean of the Stanford University School of Medicine, “if you just give me something so I can put a loud noise in my right ear.”
So Minor asked the patient to hum the particular tone. He recorded a tone of a similar frequency on a Dictaphone, played the sound in the patient’s right ear and looked into his eyes. Just as the patient had said, his eyes moved. Minor also noticed that they moved in a specific pattern.
“It wasn’t a random eye movement,” Minor says. The eyeballs, he says, move in three dimensions — vertical, horizontal and torsional (rotation about the line of sight, when described from the patient’s frame of reference) — and as he watched this patient, he paid attention to all three. The patient’s eyes moved upward and counterclockwise. The pattern never varied, and was tightly linked to the sound.
That’s essentially all it took for Minor to solve the mystery. Upon seeing the direction of the eye movement in response to this particular sound, he suspected that the source of the problem was a hole in the superior semicircular canal — one of the three tiny canals hidden deep within the inner ear. These canals serve as part of the vestibular system, a set of inner-ear structures that provides input to the brain on motion, equilibrium and spatial orientation. When just a few weeks later a second patient came to see him with similar symptoms and similar eye movements, Minor was convinced he was right.
“Both of them had very, very large eye movements evoked by sound following a similar set pattern,” Minor says. “It’s partly by chance that these two patients both had very prominent eye movements that were very easy to see.”
He had discovered a disorder that he named superior canal dehiscence syndrome — and went on to develop a surgery to treat it.
Minor was far from the only physician to see patients with bizarre sets of symptoms involving hearing, vision and perceptions of motion. At about the same time Minor was examining the eyeballs of his first patient at Johns Hopkins, a French horn player in Germany was telling his doctors that his voice echoed like a kazoo in his brain, that eating anything crunchy sounded like a gun going off. And an audiologist in Atlanta told her doctors that she could hear a loud scratching sound whenever her eyeballs moved. Both would eventually make their way, years later, into Minor’s office.
Symptoms described by these patients ranged from relatively mundane (though unpleasant) nausea and dizziness to superhero-like abilities to hear the inner workings of their own bodies — their pulse, their chewing, their digestive systems. They got misdiagnosed, underwent unnecessary surgeries, fell into depression, withdrew from the world.
“Doctors had no answers,” says the audiologist, Cindy Hirsch, AuD. “I had an eye specialist tell me this was a psychiatric case because I could hear my eyes move.”
“There was this whole bucket of patients, and we really didn’t understand what was wrong with them,” says Robert Jackler, MD, chair of otolaryngology at Stanford. “A lot of physicians thought they sounded mentally ill; they had such peculiar complaints. No one could figure out what was wrong.”
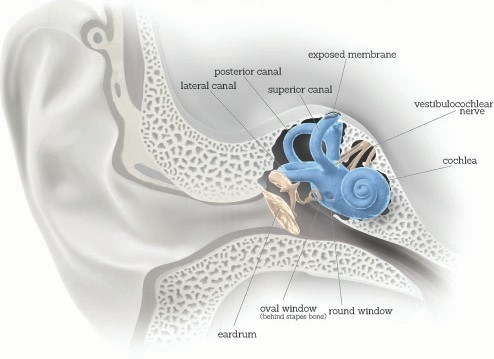
CAN LEAD TO ALL SORTS OF STRANGE SYMPTOMS
The inner ear includes the vestibular (balance) system and the cochlea, a hearing structure. Normally, it is a closed capsule with only two openings: the oval and round windows, two membranes that vibrate in opposite directions to move fluid through the cochlea, enabling it to translate sound waves into nerve impulses. But if there is an opening in the bone that should cover the superior canal of the vestibular system, the exposed membrane serves as a third mobile window into the inner ear. Sound may enter or leave through the new window, resulting in hearing problems: If it enters, it can amplify bone-conducted sounds from the body; if it leaves, it may diminish air-conducted sounds from the environment. And sounds or pressure changes in the affected ear may activate the fluid in the superior canal, causing vestibular symptoms such as eye movements, the perception that stationary objects are moving, vertigo and nausea. Illustration by Bryan Christie Design
Minor first began studying the vestibular system in a bioengineering course as an undergraduate at Brown University. Immediately, he was hooked. He was fascinated by the mathematical symmetry involved; he loved the elegant way the system worked to maintain the senses of motion and balance.
“The course used mathematical and engineering models to understand physiological systems,” Minor says. “And the professor used the balance system, and the eye movements associated with it, as an example of how you could not only describe the way the system worked, but you could learn mechanistically about how the brain was working.”
Like many scientists, Minor really likes to figure out how things work — the more complex the better. And the vestibular system is complex. Take what Minor refers to as “vestibular illusions.” Why, when you step onto an escalator that isn’t moving, does your brain tell your body that it is? Or why, when you’re sitting on a stationary train and the train next to you starts to move, does it feel like you’re moving even though you know you’re not? Unlike most of us, Minor knows exactly how complicated the answers to these questions can be.
“It was during that undergraduate course that I read the papers of the person who later became my mentor,” Minor says. That person was Jay Goldberg, PhD, now a professor emeritus of pharmacological and physiological sciences at the University of Chicago, who wrote a seminal series of scientific papers in the 1970s that captured the imagination of the young Minor. Goldberg had described for the first time the dynamics governing the responses of sensory neurons carrying information from the vestibular receptors in the inner ear to the brainstem, setting the stage for future studies in the field of vestibular neurophysiology.
Minor later wrote to Goldberg, and then traveled to Chicago to meet with him. They stayed in touch throughout Minor’s medical school years. “We made plans that I would come to work with him after I graduated from medical school.”
In between his surgical residency and a residency in otolaryngology, Minor spent four years working in Goldberg’s lab, conducting experiments in animal models that further explored vestibular neurophysiology. By the mid-1990s, as both a surgeon and an expert on the science of the vestibular system, Minor was unusually well-equipped to solve the mystery of the patients who could hear their eyeballs scratching as they moved back and forth.
‘Doctors had no answers. I had an eye specialist tell me this was a psychiatric case because I could hear my eyes move.’
The vestibular system controls how we move through the world. It works with our senses to give the brain information about where we are in space, whether we are moving, and the direction and rate of our movements. It keeps us from stumbling when we get out of bed in the middle of the night; it maintains balance and spatial orientation and keeps us from falling.
The sensory information about motion, equilibrium and spatial orientation is provided by the vestibular apparatus, which in each ear includes the utricle, saccule, and those three semicircular canals, bones so small that together they can fit on the surface of a dime. The utricle and the saccule, two sacs located just below the semicircular canals, contain small stones and viscous fluid that enable hair cells to detect linear motion and orientation relative to gravity. The saccule and utricle detect vertical linear motion, like when you drop in an elevator, and horizontal linear movement, such as zooming forward in a car. The fluid-filled semicircular canals detect rotational movement and inform the brain about angular head movements.
Each of the canals lies along a different plane, perpendicular to one another, and sends messages to the balance center in the brain for head rotation in its plane. When the head rotates in a direction sensed by a particular canal, the fluid within it lags behind because of inertia and exerts pressure against a specialized structure — the canal’s sensory receptor. The receptor then sends nerve impulses to the brain about movement from the specific canal that is stimulated.
One of the most important functions of the vestibular system is to keep the eyes focused on objects of interest during head movements, like when you’re driving down a bumpy road. Rotatory motion upward and downward is where the superior semicircular canal comes in. As Minor knew from studying late-19th-century experiments on the vestibular system in pigeons, pressure on the superior semicircular canal causes the eyes to move in the plane of that canal. It was this motion that Minor saw when he watched his two patients’ eyes move in response to sound, and suspected that it must be the superior canal that was damaged.
“The specific pattern of the eye movements, that was a smoking gun pointing to the superior semicircular canal being the source of the problem,” Minor says.
Normally, the inner ear is a closed capsule with only two openings — the oval and round windows of the cochlea. Having a hole in one of the canals — a third opening — can lead to a number of auditory and vestibular disturbances. Among the most dramatic: Sounds from inside the body can enter directly into the inner ear through bone conduction.
“Some of the sounds that are already in our body, our pulse, our neck creaking, our own voice, those get into the inner ear through that hole much more readily than normal, so people report these crazy symptoms like hearing their eyes move, hearing their blood,” says John Carey, MD, one of Minor’s colleagues at Johns Hopkins who assisted in the later surgeries and research. “It may be too loud or distorted because they are hearing their voice come through their bones directly into their ear. Their voices sound loud, uncomfortable, distorted. Many patients resort to whispering.”
To test his theory, Minor and colleagues collaborated with a neuroradiologist to develop a more sensitive version of a CT scan to search for a tiny hole in the canal.
Within months, they were able to scan the gentleman who liked to sing in the shower. Sure enough, there was a hole in his right superior semicircular canal.
Finally, an answer.
“In addition to being sent to a psychiatrist and told that he was imagining these things, which he clearly wasn’t, the patient was concerned that maybe he had multiple sclerosis or a neurological disease,” says Minor. “For him it was just a real frustration. Once we figured out what it was, he felt reassured and did not feel he needed the problem to be corrected. He just stopped singing in the shower.”
About two-thirds of patients with the syndrome choose to live with it; others have symptoms that are just too disabling, Minor says. They want a cure badly.
His second patient, also at Johns Hopkins, fit into this category. Like the first patient, she had sound-induced wobbling vision known as oscillopsia, but she also had disequilibrium.
Minor and his colleagues at Johns Hopkins developed an operation to correct the disorder. The surgery entails making an incision above the ear and then gently elevating the temporal lobe of the brain to reveal the superior canal, using fascia and bone to plug the canal hole, securing the opening in the skull with titanium plates and sewing the scalp back up. Other surgical approaches to correct the disorder have also been developed in the intervening 20 years.
In 1996, he operated on his second patient and her symptoms immediately disappeared. In 1998, Minor and colleagues at Johns Hopkins published their first paper on the disorder, in the Archives of Otolaryngology Head and Neck Surgery, describing eight patients with the syndrome. A series of additional publications followed.
“We showed that there were specific hearing abnormalities associated with the syndrome,” Minor says. “We also showed that there were other vestibular abnormalities that could be evaluated by clinical tests. We established that the surgery was selective in its effects on the superior canal. That the sound-induced eye movements went away. That the hearing often returned to its normal range. Most of the severe symptoms were gone. Patients were much better than before. In making these discoveries, we also extended our understanding of vestibular physiology. Our work on this syndrome has been a wonderful synthesis of bench to bedside and back to bench.”
Exactly how many people suffer from this syndrome remains unclear, Minor says. At Johns Hopkins, surgeons have performed about 240 procedures, and they are often done at Stanford as well. What is known: Many patients are diagnosing themselves online. Both the audiologist from Atlanta and the horn player from Germany found out about Minor’s research and discoveries online, then contacted him at Johns Hopkins by email. Minor eventually operated on both. Some have suggested the disorder be renamed Minor’s syndrome.
For the horn player, surgery ended 22 years of suffering. He was able to return to his music. Hirsch, the audiologist, had endured the syndrome for seven years.
“My symptoms kept getting worse,” she says. “I stopped attending weddings, bar mitzvahs and my children’s sporting events. I became a social recluse. In November 2004, I went searching for answers online, found Dr. Minor and emailed him. He called me that night at 5 p.m. on a Friday. I was overwhelmed and honored to hear directly from him.”
On Feb. 10, 2006, at Johns Hopkins, she became the 34th patient with superior canal dehiscence syndrome to have canal-plugging surgery. After waking up from surgery, the surgeons asked if she was OK. She motioned with her hand for them to wait, then closed her eyes and moved them back and forth. There was no sound. Her eyeballs had been silenced.
