
Sound research
Scientific innovations harness noise and acoustics for healing

From the original stethoscope, invented more than 200 years ago, to the fleeting chirp of gravitational waves, sound has reverberated throughout the history of technological and scientific advances.
Today, the role of sound in science extends beyond the range of audible frequencies: Ultrasonic and other silent acoustic waves have made their way into researchers’ repertoire, helping them push the boundaries of conventional medicine and research.
In examples from four Stanford labs, scientists are investigating the full spectrum, harnessing the nuances of noise and the power of acoustics to generate inventive, if not unexpected, technologies that show just how potent the combination of sound and science can be.
Turning the irksome into the advantage
Nothing incites irritation in quite the same way as a lurking mosquito. But its high-pitched drone may actually help curb spikes in mosquito populations and, more importantly, the diseases that they pass on to humans. This, at least, is the premise behind Manu Prakash’s newly launched app, Abuzz.
Prakash, PhD, assistant professor of bioengineering, created Abuzz to digitally identify and tag mosquito species based on their hums. His vision: build a “soundscape” that maps the global whereabouts of these voracious vectors and provide details about the diseases they can carry — Zika, malaria, dengue and the like. It may seem lofty, but Prakash asserts that all he needs is an avid user base with access to cellphones (“dumb” phones like a flip phone make the cut).
“Our goal is to put the data in the hands of locals and public health organizations who are focused on mosquito-disease elimination,” Prakash says. “We want this to provide details of mosquito ecology — species, associated diseases, the location of the recording — so that it can be a worldwide awareness and alert system for disease-carrying mosquitoes.”
Naturally, populating such a map will take time, and a lot of users. So how does one collect that much data from far-flung corners of the globe? Recruitment and a simple training session, Prakash says, that consists of four basic steps: venture out, creep up to a mosquito (or let it creep up to you), record its pitchy hum and send the data to Abuzz for analysis.
“What’s beautiful about Abuzz is it’s not just limited to mosquitoes. Right now, we’re looking into whether we can use this method to identify sick versus healthy honeybees.”
Abuzz — the Shazam app of the insect world — uses software to determine if the recorded noise is really a mosquito, not a house fly, distant jet or other imposter. Then, it compares the recording with a database of different mosquito buzzes and tries to find a match. This is possible because every mosquito species emits a unique sound, generated by the flutter of its wings.
Ideally, knowing the geographic regions where specific mosquito species are recorded can help battle unwanted multiplication. “Locals could look in their neighborhood for likely mosquito-spawning areas and remove the larvae,” Prakash suggests.
Or, on a larger scale, agencies that try to hinder populations by releasing genetically modified mosquitoes could use the information to more precisely target regions and species. (Releasing an army of mosquitoes into the ether may sound rather vile, but gene modifications in these mosquitoes make their offspring unviable, helping to curtail a climbing population.)
“What’s beautiful about Abuzz is it’s not just limited to mosquitoes,” says Prakash. “Right now, we’re looking into whether we can use this method to identify sick versus healthy honeybees.” They don’t have the answer, but as health of honeybees in the United States continues to decline, Prakash and his team hope that their platform can help reveal the biology behind more than one flying insect.
Acoustic choreography
Heart cells are among the most densely packed in the body — about 100 million fit into a space the size of a sugar cube. The compact structure crams the cells so close together that they can communicate with one another and beat as one lump. For tissue engineers, however, it poses a tricky hurdle: Pack the cells too tightly and some won’t get proper nutrients; too loosely and they can’t coordinate a beat.
Cardiologist Sean Wu, MD, PhD, had been probing the problem when he met Utkan Demirci, PhD, an acoustic bioengineer and professor of radiology. “Utkan brought up this idea that we could use acoustics to pack the cells very densely and still maintain an ability to control and tune their organization — and we got really excited,” says Wu, associate professor of medicine.
Demirci’s idea exploits a type of acoustic signal that creates Faraday waves, which result from a physical perturbation at the interface of liquid and air (if you’ve ever flown in a turbulent plane with a beverage, you’ve witnessed Faraday waves in your cup). The waves cause ripples in the liquid, and anything floating in the liquid sloshes around too.
“You can trigger those ripples on the microscale,” explains Demirci. “Like when the tides of the ocean sweep a sunken ship’s treasures to shore — we’re sort of doing the same thing with heart cells.” The big difference, however, is that Demirci and Wu can control the “swell” by tuning a knob that changes the waves.
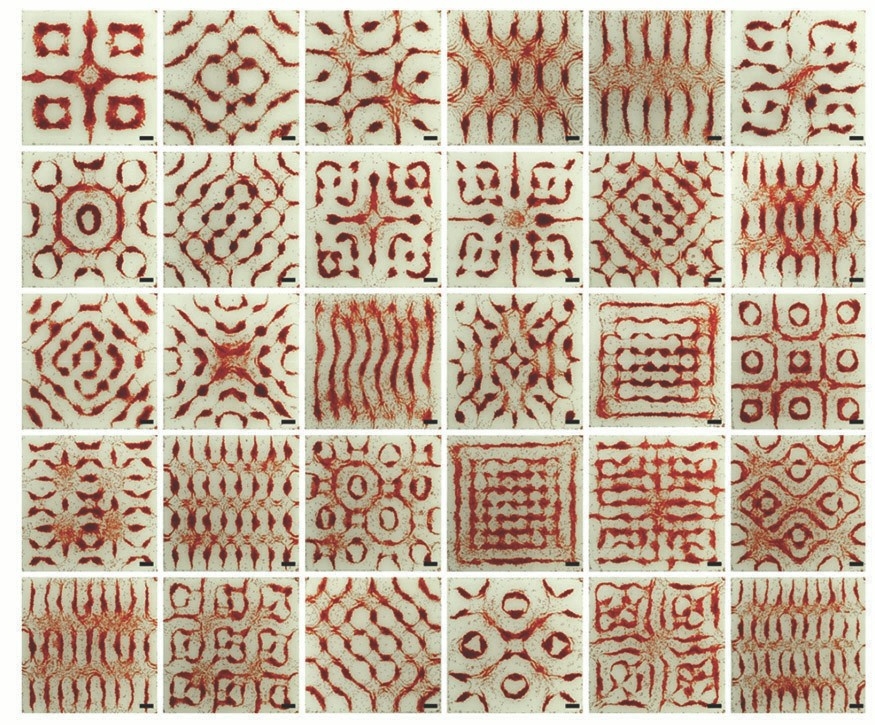
Wu and Demirci can then shepherd the heart cells into nearly any pattern they want. “You can make triangles, hexagonal shapes, circles, lines — you can even make a little human shape,” Demirci says.
“And,” Wu adds, “if you don’t like the pattern, for whatever reason, you can change it, literally, within five or six seconds. You change the frequency and amplitude, and the cells move into a new spot right in front of your eyes.”
Unlike other tissue engineering tactics, acoustics position the heart cells in a tight configuration that closely resembles natural cardiac tissue, turning the resulting, beating blob into something valuable for medicine.
Wu and Demirci think acoustic engineering could help foster more realistic cardiac disease modeling and drug screening. More distantly, but still on the horizon, the pair even see their generated tissue as an option for heart patches in patients who have weak cardiac walls or have damage from a heart attack.
Next, Demirci and Wu say that they plan to add vascularization — conduits that carry blood and oxygen to various parts of an organ — to make their generated heart tissue even more realistic.
A symphony in the brain
While listening to a string quartet play over recordings of plasma waves captured in outer space and converted into sound, neurologist Josef Parvizi, MD, PhD, dreamed up a symphony of his own. If you can turn signals from space into sound, perhaps you could turn brain waves into sound too, he thought.
So Parvizi sent an out-of-the-blue email to Christopher Chafe, a composer with expertise in converting atypical data sets into music, and explained his vision. Parvizi, professor of neurology, describes what happened next: “A crazy music professor and a crazy neurologist decided to collaborate on a strange idea.” Chafe is the director of Stanford’s Center for Computer Research in Music and Acoustics.
After several years of refining, the idea developed into something that Parvizi has dubbed the brain stethoscope.
The instrument, which is noninvasive and looks like a sweatband, straps onto a person’s head and listens to the brain’s electrical signals. With a push of a button, those signals are converted to sound that streams from a small speaker connected to the band. The thought is that doctors can “hear” the tone of the brain — particularly if there is a seizure.
“Imagine that you open a hotel room window and the entire town is chanting exactly the same thing,” says Parvizi. “You may not know exactly what’s happening, but you know it’s not normal. It’s the same idea with the brain; you don’t want signals to be too synchronous. If they are, the brain is having a seizure.” It turns out, the audible difference between a seizing brain and a normal brain is quite distinct; almost anyone can hear it.
“You want moms and dads to be able to know if their kid is having a seizure so that they seek out professional attention.”
Of course, Parvizi acknowledges, if someone is convulsing and shaking, you don’t need a stethoscope to tell you they’re having a seizure. “But there’s such a thing as ‘non-convulsive subclinical seizures’ and those don’t have the obvious physical symptoms.”
But they still have some subtle symptoms. Someone having one of these silent storms might appear disoriented and nonresponsive, or they might fall asleep suddenly. In the public eye, this type of seizure more often flies under the radar, but that’s not to say they’re less threatening to health. Parvizi says there’s now a stockpile of evidence showing that prolonged silent seizures are damaging to the brain, especially in children, whose brains are still developing.
“Right now, patients need a trained neurologist to detect a seizure. It may be controversial, but my goal is to enable anyone to detect them — all kinds of physicians, nurses, medical trainees.”
Even parents.
“You want moms and dads to be able to know if their kid is having a seizure so that they seek out professional attention,” Parvizi says.
In May 2017, the FDA gave the green light to Parvizi’s invention, and he has since tested the stethoscope’s capabilities in several hospitals, finding encouraging results.
“This could change health care dramatically when it comes to monitoring brains.”
Powering implantable medicine
Place two grains of rice next to each other and you’ve about replicated the size of a rather savvy, next-generation medical chip devised by Amin Arbabian, PhD, assistant professor of electrical engineering. The chip is an implantable device, like a pacemaker or nerve stimulator, but is set apart by the way it’s powered — not by batteries or wires, but by sound.
“It has been a long-standing challenge to make medical devices as small as possible and operate deep in the body,” says Arbabian. “Ultrasound enables that.”
Ultrasound’s long-term use in fetal imaging has earned it a reputation in medicine for being safe and dependable, making it a prime candidate to power a chip that can be embedded in the body. Perhaps equally as important, the gentle sound waves also support versatility. A Swiss army knife of implantable devices, the chip can change its function to fulfill different biological needs. Its various modes are controlled by the same thing that fuels it. “Ultrasound is both a power source and a way to communicate with the device,” says Arbabian.
A tiny module, called a harvester, sits on the chip and converts ultrasound waves into electrical energy. By beaming pulses of ultrasound to the chip, Arbabian can send encoded commands, like Morse code. “We can, for example, instruct it to start monitoring a certain parameter, like blood pressure, or channel an electrical pulse to stimulate a nerve or trigger the precise release of a drug at a particular location.”
“We could see this system working for maintaining blood pressure, or managing urinary incontinence or diabetes.”
The goal, he says, is to create an active “smart” chip or a distributed network of smart chips to not only execute specific commands, but also to monitor physiological parameters and transmit useful data about the patient. This information, on such things as insulin levels or blood pressure, is sent to an external device, where doctors can access it. In that vein, Arbabian and his lab team are working toward a closed-loop system in which the implant is self-sustaining and can run seamlessly in the body, without constant instruction.
In a closed-loop system, the chip’s sensors would trigger the release of a dose of its therapeutic agent, which could be an electrical pulse or a drug enclosed in a separate chamber of the chip. In patients with hypertension, for instance, the implant would monitor the arteries. If the chip sensed increased blood pressure, it would administer a drug to help bring the pressure down.
“We could see this system working for maintaining blood pressure, or managing urinary incontinence or diabetes,” says Arbabian.
He and his team are working on the next generation of the implant and partnering with other labs to test their setup in animals. They even have a research collaboration with the FDA, which is independently investigating the prototypes.
“There’s a lot more work to be done,” Arbabian says. “But there’s a lot of reason to be hopeful.”
