
Fever pitch
When science collides with politics

Two years ago, Ebola jumped from the jungle into West African cities and ultimately the United States. As a physician-journalist for ABC and NBC News, I had covered tough stories around the globe — from epidemics to wars and refugee camps. But nothing prepared me for the drama and sociopolitical fallout from Ebola. We had all been watching the devastation from this epidemic play out from a distance in print and on television. With each compelling story, Ebola became increasingly tragic and exotic, yet it was safely oh-so-far away.
And then Thomas Eric Duncan brought everything home. The Liberian man who arrived in Dallas on Sept. 20, 2014, was infected with Ebola, and within hours of his hospitalization, a nation was on edge. For all the upheaval that was to follow, it is important to look back and remember that he remains the only person to have died of this disease in the United States. Two health-care workers who cared for him became infected but survived, and none of Duncan’s family members contracted the disease. Yet Ebola held America hostage.
The arrival of Ebola on U.S. shores set up a collision of science, politics and public trust unlike anything we had ever witnessed in public health. People exhibited great distrust and, ultimately, disregard of the government and institutions like the Centers for Disease Control.
Health officials struggled to calm people and keep the message on track: that Ebola is spread through direct contact with bodily fluids, that only symptomatic patients are contagious and that the virus would be contained in a country with the medical and public-health infrastructure of the United States. But every day, with the help of a ravenous 24-hour news cycle, the truth got derailed. The fear that Ebola would sweep across the United States, however improbable, was palpable.
Duncan’s family was appropriately quarantined in their apartment because they had been in contact with him after he developed a fever, vomiting and diarrhea. No one entered or left the premises. Soon, however, the word “quarantine” would be used loosely and sloppily, adding a new layer of confusion.
My NBC News team and I left for Liberia on Sept. 26, one day after Duncan was seen in a Dallas ER and sent home febrile with antibiotics. He returned three days later, critically ill, and was hospitalized. While Dallas would soon become the center of attention for most Americans, I believed the real story was still in Liberia. I thought if I could explain what was happening at the epicenter of the epidemic, we could quell people’s fears at home. I was wrong; soon my team and I would become part of the story and complicate the narrative even more.
While in Liberia, we hired a young American journalist, Ashoka Mukpo, who had spent a lot of time in Monrovia, the capital city. He was on the team for less than a day when he developed a fever. After malaria was ruled out, Ebola was confirmed and within days he was on a chartered flight to the University of Nebraska Medical Center. My team stayed in Liberia and we continued to report for several days before it was time for us to come home. For all the devastation I witnessed on the streets of Monrovia, where every day people lived in constant fear of contracting Ebola or losing a loved one, I was blind to the persistent fright in the United States.
The cardinal rule in Liberia was to touch no one — no exceptions. We took our temperatures four times a day and reported them to one another. We all kept our distance — 4 to 6 feet was the norm and that was true of my interactions with Ashoka. While working with us, his temperature was normal, which meant he was not contagious. His fever didn’t develop until hours after leaving one evening; after that, all contact was via phone or text. But once the word was out that a “member of an NBC News team has Ebola,” the media firestorm began. There were tweets calling for us to be detained in Liberia.
I was warned by my colleagues that rhetoric on the homefront was increasingly angry and fearful, with some voices clamoring that allowing sick people, or even healthy journalists, back into the United States could put people at risk. But I knew the science told another story. And I had seen our country face infectious diseases before — influenza, polio and HIV/AIDS. Each time we emerged stronger, smarter and more thoughtful. We became better doctors and scientists and more compassionate citizens. But those epidemics had one thing in common. They occurred before social media was an entity.
The staff at Nebraska Medicine knew that accepting an Ebola patient would set up a scenario that would need to be handled like nothing they had experienced before. The medical team had been practicing for 10 years to contain such a deadly infectious disease, and the doctors knew that messaging would be as important as the quality of the medical care. So while Dallas was bleaching sidewalks, this medical community in America’s heartland addressed the public immediately. Daily press conferences served to teach and allay fears and invited the community to trust their doctors and institutions and be proud about the work that was being done. The doctors said, “We built our bio-containment center for this kind of emergency. We want you to know that the public is not at risk. We will be speaking with you every day.” They kept their word.
Life in Omaha remained calm and normal. The doctors and nurses who spent days with the infected patients took showers after their shifts, changed back into their street clothes and went into their communities — grocery shopping, attending school plays and having dinner with their children. Instead of fear and shunning, these brave health-care workers were met with love and support. Science, impeccable communication and compassion prevented politics and bad policy from hijacking the work at hand. To this day, people in Omaha speak of the pride they have for the role their city played in treating the Ebola patients.
Back on the East Coast the language was anything but tempered. While Ashoka remained in Omaha, I was home in New Jersey, housing two of my NBC colleagues. Our bosses had warned us that the rhetoric around Ebola was escalating in the United States but I was not taking their concerns to heart. Ebola may be a flamboyant virus and an attention getter but I knew it wouldn’t sweep across the country.
We arrived home to public health chaos. The New York State Department of Health disagreed with the New York City Department of Health, which differed from the New Jersey Health Department. And no state body wanted to follow the CDC guidelines. Each of us had been interviewed by a CDC official in Monrovia, cleared for travel and given a risk score of zero. To me, the CDC guidelines were the most important: to monitor our temperatures twice a day, report in with our local health official, and avoid large gatherings like churches and grocery stores. We need not be confined. That made sense to me. But states are not required to follow federal guidelines, and common sense was not ruling the day.
Several days after being home, I was seen in my car and a woman anonymously dialed 911. That call triggered the New Jersey State Police who reported the event to Gov. Chris Christie. With all the mistakes that had been made in handling Duncan in Texas, I believe that Christie wanted to set a different example. And what better way to address Ebola than to crack down and say, “Not in my state.”
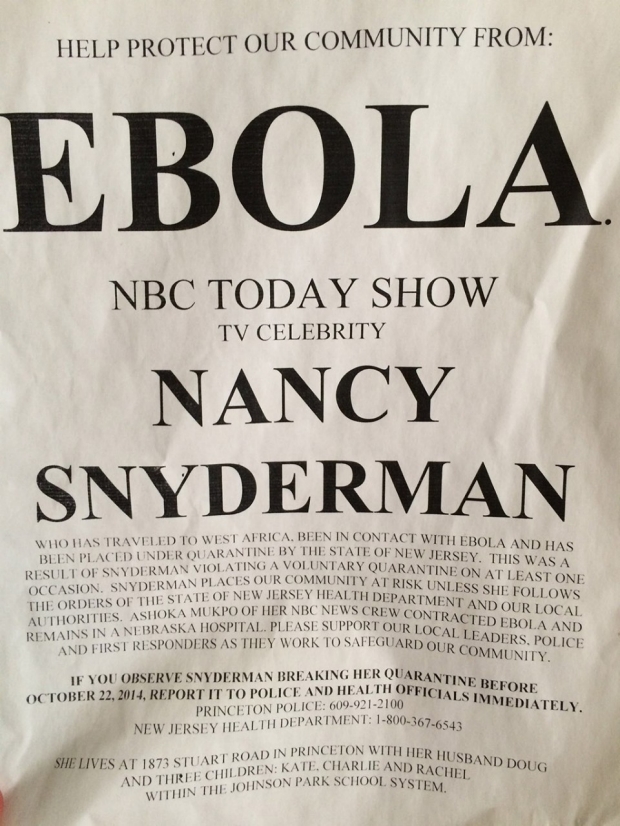
At 10 p.m. on a Friday my team and I were served with papers confining us to my house. The word “quarantine” was used but not in a scientific way. While the three of us were confined to the premises, other people were allowed to come and go — which made no sense. Quarantines are not porous. The fallout was insane. Because my 89-year-old mother had been in my house — she brought us groceries — Princeton’s senior center would not give her a flu shot. “Wanted” posters were placed on public kiosks with my children’s names and our address, urging people to keep an eye on us. It was ugly and frightening. Even the town council, while agreeing that the posters were offensive and dangerous, declared that they were protected by the First Amendment.
A few weeks later, on Oct. 24, Gov. Christie detained Kaci Hickox, a nurse returning from working with Ebola patients in Sierra Leone, and held her in a tent at Newark Airport, despite the fact that she was afebrile and posed no threat to the public. Her clothes were taken from her and she was given hospital scrubs; her bathroom was a port-a-potty. It was not a very flattering view of the hospital capabilities in New Jersey. But the message was strong. “Not in my backyard. I don’t need the CDC’s advice. This is how we are handling it.”
Today, Ebola is a distant memory and Zika is the medical headline of the day. Ebola exploded, liquefying bodies and destroying countless lives, and just as suddenly retreated into the African bush. But it will be back. Viruses, once they make themselves known, do not go away.
Which brings as to Zika and the reality that this virus has come to American shores to stay. As with Ebola in the early days, we watched from afar and wondered what would happen. But while Ebola burst on the U.S. scene, Zika trickled. That trickle allowed the CDC to get ahead of the messaging, and television network reporting was measured. In real time we all tracked the movement of mosquitoes to Brazil and Puerto Rico and finally Miami.
And this time we have a vector as an enemy. We can hate mosquitoes, fear them and not each other. A virus in an insect is somehow less terrifying than a virus in a person who has traveled from afar. Zika is not flamboyant. It has no movies or popular books to help conjure up images of bodies liquefying. It caused a flurry of handwringing around the Rio Olympics, but the Games went on and there were no reported cases of infection. Now winter is upon us, and we can hope that mosquitoes in North America will die their usual seasonal deaths. And so it goes.
But have we really learned anything about the dangerous interference of politics with medicine? While President Obama and National Institute of Allergy and Infectious Diseases director Dr. Tony Fauci implored Congress to release funds for Zika vaccine research, Congress instead left for summer break, putting clinical trials of a vaccine and hopes of fast-tracking it in peril. A line in the bill allowing Zika funding to be used in Planned Parenthood clinics along with other community health centers was enough to stall the allocation of funds. Congress finally approved Zika funding of $1.1 billion in late September.
We are becoming a scientifically illiterate nation, and rising populism fuels distrust of our nation’s scientists and revered institutions. Politicians add to the mess by denying evolution, vaccine safety and climate change. Our failure to address Ebola and Zika with a sound scientific discourse hurts us far beyond these two outbreaks. It does nothing to quell the anti-science, anti-immunization zeitgeist, which puts our vaccination programs at further risk and chips away at our public health system.
Viruses don’t care about walls, or bad politics, or frightening rhetoric. The next viral outbreak that Americans have never heard about is just around the corner. We can’t afford to let good science, public safety and global health be hijacked by politics. The public has a right to accurate information, rather than fear-mongering. Physicians who serve in Congress need to be better leaders, and the press has a responsibility to push for truth and follow the science. Science is not linear, and the scientific process can be messy — just like democracy. And that makes our collective responsibility all the more important.
Nancy Snyderman, MD, is a consulting professor with Stanford’s Center for Innovation in Global Health. Contact her at medmag@stanford.edu.
