
Eye spy
Looking inside the eye with technology once turned to the sky

“What are you going to do for my son?” the woman asked.
It was 2007 and the researcher in the hot seat was physicist Alfredo Dubra, PhD, then a research associate at the University of Rochester in New York. Dubra was pioneering new ways to peer into the human eye to identify damage to the light-sensing cells that make up the retina.
As part of his research, he’d just examined the woman, who was suffering from an inherited retinal disease. She had already lost most of her sight, and Dubra knew that a similar fate likely awaited her teen son.
“In that one moment, that single question fundamentally changed the way I do research,” Dubra recalls. “That moment is imprinted upon my memory.”
In the years since, Dubra, now an associate professor of ophthalmology at Stanford, has become a leader in the field of adaptive optics — an imaging technique that uses Cold War-driven advances in astronomical telescopes to view a whole new galaxy of cells and anatomical structures in the human eye.
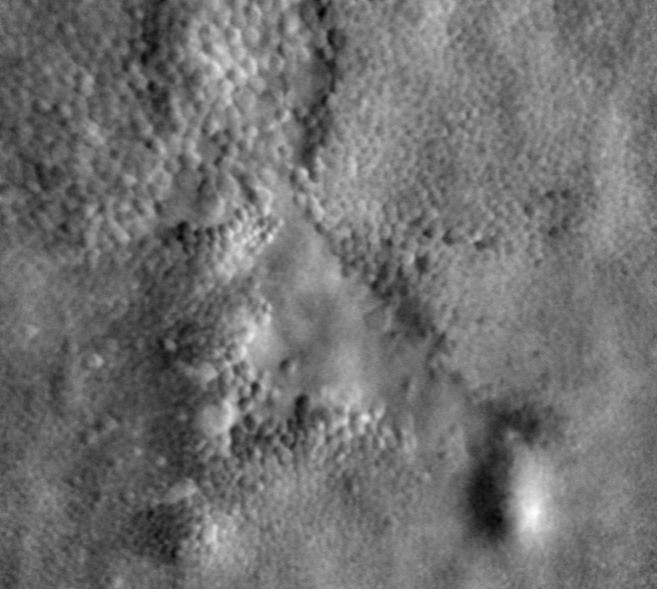
Normally these cells, closeted at the back of the eye, are surprisingly hard to see in any fine detail. But adaptive optics transforms blurry, gray images reminiscent of static on a poorly tuned television into a clearly defined landscape in which an individual cell’s structure, location and even functional status can be determined. It’s likely to change lives by permitting researchers and clinicians to diagnose, monitor and treat devastating, degenerative retinal and neuronal diseases earlier and more effectively.
“The advances that Alf and his team have made in adaptive optics have changed the way we in the field look at photoreceptors in the retina,” says Michel Michaelides, MD, professor of ophthalmology at University College London and one of the leaders of the UCL gene therapy trial pipeline for inherited retinal diseases. “There really is no parallel for the quality of images we can now see.”
More than 10 million Americans are affected by as-yet-incurable vision loss, and Dubra is quick to connect the dots between these people and his lab’s (and life’s) work.
“I will never forget that woman and her son,” Dubra says. “All too often patients are just abstract concepts to physicists and engineers like me, and it’s easy to stay immersed in the technology and forget the end goal. That’s why it’s vitally important to have regular contact with people who are visually impaired, and who desperately need help. These people are going blind.”
“I will never forget that woman and her son. All too often patients are just abstract concepts to physicists and engineers like me.”
Through a child’s eyes
Not long ago, Dubra, who was born and raised in Uruguay, was one of those people. As an infant, he suffered from a severe case of strabismus, or crossed eyes. He needed several surgeries before age 3 to correct the misalignment and ensure that the visual cortex of his brain learned to properly interpret the signals around him. Untreated, strabismus can lead to blindness if the developing brain abandons attempts to decipher images from the affected eye or eyes.
“When I was about 7, I was leaving a visit to the eye doctor to see how my eyes were developing, and I burst into tears,” says Dubra. “My father tried to find out what was wrong, and I finally told him, ‘This guy is never going to be able to fix me; he wears glasses!’
“My father said, ‘Well, you know, sometimes people decide to base their careers on things related to problems they themselves have experienced.’” Dubra’s grandfather, a cardiologist in Uruguay, had chosen his career in response to his own heart problems. Then and there, Dubra decided to devote his life to learning more about the eyes and how they work. But his early plan of attending medical school was thwarted when his middle school biology teacher brought a dead fish to class for dissection.
“Immediately I knew, ‘No, I can’t go into medicine,’” Dubra recalled. So he chose a different but related path important to vision: physics.
How vision works
The fundamentals of vision are this: Light enters the eye, which is roughly the size and shape of a ping-pong ball, through a thin layer of tissue called the cornea. The cornea begins the process of focusing the light as it enters through a hole in the iris called the pupil. Immediately behind the pupil, the light passes through a lens that serves to focus the light onto a layer of light-sensing cells at the back of the eye — the retina. The optic nerve then transmits signals from cells in the retina to the brain to be decoded as visual images.
The retina lines the inner three-quarters of the eye; laid flat it would be a little bigger than a quarter. It’s peppered with cone cells (which discern the colors red, green and blue), rod cells (which allow us to see in dim light, but don’t perceive color) and retinal ganglion cells (which connect the rod and cone cells to the brain via the optic nerve). Humans have about 120 million tiny rod cells and about 6 million larger cone cells.
Diseases that affect vision can occur in the cornea, lens, retina, optic nerve or even the brain. But although the cornea and lens can be replaced with donated or synthetic tissues, the retina and the optic nerve are much more precious.
“The retina is a direct outgrowth of the brain,” says Dubra. “Almost all the cells in the retina are neurons. And, like neurons in the brain and spinal cord, when they die, they don’t get replaced. That cell loss is permanent.”
Unfortunately, it’s also insidious. The first stages of many retinal diseases are gradual and unnoticeable; most people don’t discover any vision changes until a critical mass of cells are lost. And although some gene therapy approaches have shown promise in replacing faulty or missing copies of proteins that keep the retina healthy, the technique falls flat when the cells themselves are missing.
“You can’t cure cells that aren’t there,” says Dubra. “That’s why diagnosing these diseases as early as possible is the goal of every ophthalmologist. But by the time a person notices vision impairment, thousands of cells are likely to have died.
“Although many of these diseases are currently incurable,” he adds, “in some cases there are drugs that can slow their progress. If we could diagnose them early, and treat them throughout a person’s life, vision loss that significantly affects a person’s quality of life could be prevented. Ideally we would also be able to monitor whether a chosen therapy is working, or if a different therapy or drug should be tried.”
Adaptive optics arose as a result of the cold war, when U.S. Military specialists were eager to track Russian spy satellites orbiting high above the Earth.
So how can we monitor individual rod and cone cells in the retina? It might not seem like a big deal. After all, we routinely image cells outside the body using high-powered light or even electron microscopy. But Dubra and his colleagues need to visualize the living cells of retina. This presents particular optical challenges.
All of us see objects by collecting, focusing and interpreting the patterns of light that bounce off of them and reach our eye. Our brains learn how to compensate for the vagaries of our individual eye structure to determine whether one wavy pattern of light reaching our retinas is our family dog waiting lovingly by the back door, or a dangerous mountain lion lurking in the bushes along our evening running route. Sometimes this interpretation is improved with the help of eyeglasses or contact lenses to correct for common deformities.
From outer space to the eye
When it comes to looking at the retina itself, however, the tables are turned. Now the clinician is trying to interpret light waves bouncing off the patient’s retina as they retrace their steps out of the eye, passing through the lens and cornea and even the veil of protective tears that cover the eye’s surface. Each of these obstacles can jumble the waves of reflected light and make fine details difficult to discern. It’s a bit like trying to identify the individual pixels on this page by looking through a wavy piece of glass, or while underwater without goggles.
What’s more, each patient is unique, from right eye to left eye and even from moment to moment as the eye is repeatedly wetted with each blink.
These complications could be avoided if the retina could be removed from the eye and examined directly in the absence of tears, cornea, lens, etc. But that’s obviously not the preferred approach for a patient who ever wants to see again.
In short, looking at the retina at any level of fine detail is challenging. Unless, that is, you’re familiar with outer space and international intrigue.
Adaptive optics arose as a result of the Cold War, when U.S. military specialists were eager to track Russian spy satellites orbiting high above the Earth. But atmospheric distortion of the light reflected from the satellites limited what telescopes on the ground could see. This distortion is the same reason stars appear to twinkle.
“Light waves from those stars travel many light years to reach Earth, and then at the last small fraction of a second they enter our atmosphere,” says Dubra. “Pockets of hot and cold air act as lenses that bend these rays of that light and make the images of the stars appear blurry or flickering.”
The effect is similar to the visual distortions we’ve all noticed when looking down a long, empty stretch of highway on a hot day, or gazing at someone across a bonfire. The air itself appears wavy and details are difficult to pick out.
“Now imagine if you had a magical device that could intercept these distorted light waves and correct them,” says Dubra enthusiastically. American astronomer Horace Babcock, PhD, came up with just such an approach in 1953 when he suggested bouncing the distorted waves off a deformable mirror. Linking the mirror to a device that could sense the distortion would then allow the mirror to repeatedly and quickly adjust as necessary to realign the light waves and re-create a sharp, visible image.
The idea worked, and military researchers spent decades optimizing this “adaptive optics” technology as a way to better track Russian spy satellites far above the Earth.
When the Cold War ended in 1991 with the fall of the Soviet Union, the military declassified their work on adaptive optics, and medical researchers quickly realized the technique’s promise for peering into the inner space of the human eye. And by 1997, researchers at the University of Rochester’s Center for Visual Science — including Junzhong Liang, PhD; David Williams, PhD; and Donald Miller, PhD — published the first paper showing that adaptive optics could allow them to see individual cone cells with “unprecedented resolution.”
‘I had to leave’
At about the same time, Dubra, who was finishing up his undergraduate studies in physics in Uruguay, was coming to a bleak realization of his own. “At some point, I came to understand that we were never going to study the eye here. There were just no researchers in this country specializing in the physics of vision. So I had to leave.”
After finishing his master’s degree in 2000, Dubra headed to the United Kingdom to complete a doctorate and postdoctoral studies at the Blackett Laboratory in Imperial College London, where he designed and built a machine to study the topography of the film of tears that cover the surface of the eye with each blink.
In 2006 he packed his bags to join Williams’ laboratory in Rochester. “David’s team pioneered adaptive optics for retinal imaging,” says Dubra. “So there was a unique opportunity to learn about vision science while also further advancing the imaging technology.”
In 2011, Dubra, who was then an assistant professor of ophthalmology at Rochester, hit upon a way to change the three-dimensional orientation of the series of imaging mirrors in such a way that it became possible to visualize not just cone cells, but also the much smaller, and more numerous, rod cells. This was a major technical achievement.
“We and others had thought that these cells were far too small for us to see in the living eye,” says Dubra. “But many diseases start in these rod cells and then propagate to other cell types. So imaging them is very important.”
“Alf has a rare ability to interact with both scientists and clinicians to develop the technology necessary to help us help patients.”
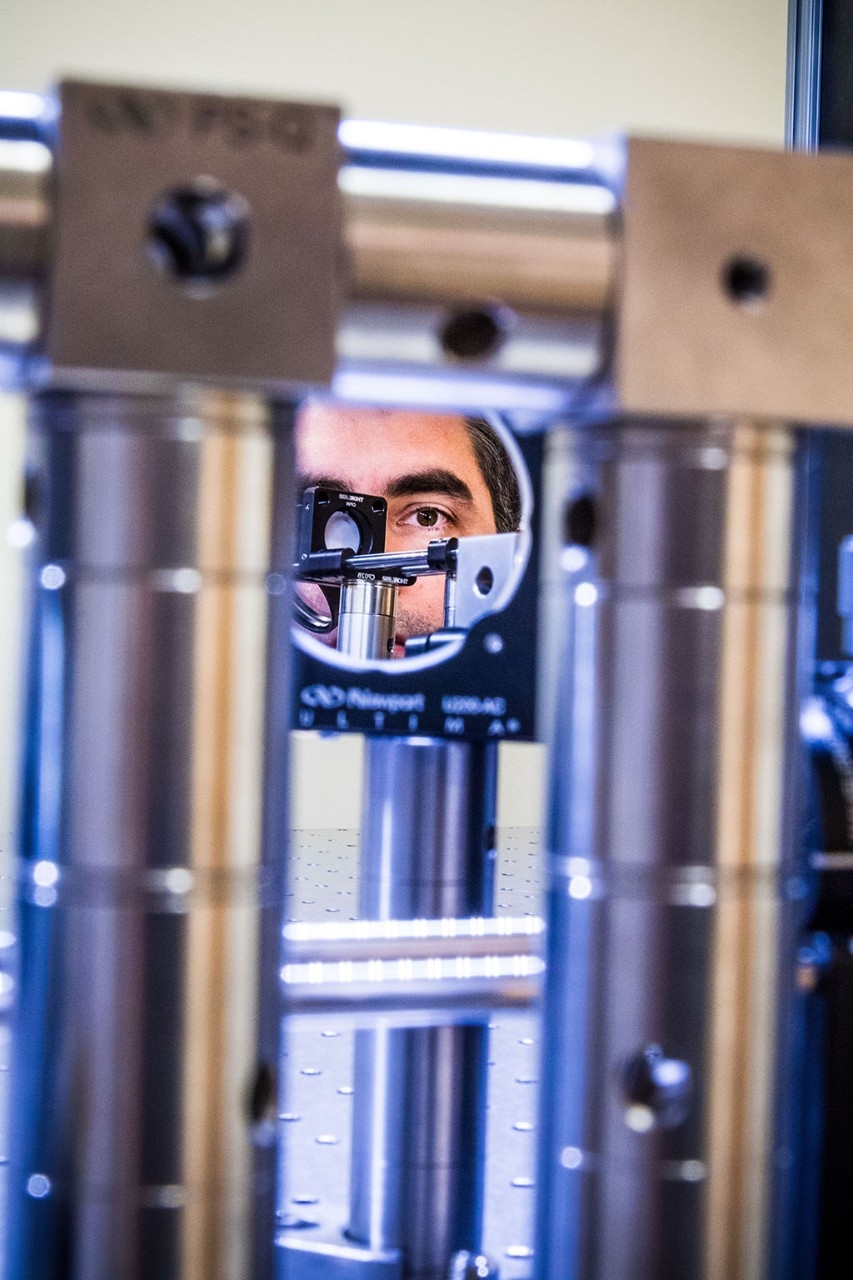
If the human eye is about the size of a ping-pong ball, the machines that Dubra and his colleagues build are roughly the size and shape of a thick ping-pong table. The patient sits at the end of one of the longer sides and aligns their eye with the machine by resting their chin on a support and peering into a box built onto the top of the table that looks somewhat like an old-style film camera with a photographer’s hood. The retina is illuminated with light that enters the pupil of the eye; a series of mirrors and detectors housed under the protective cover correct, focus and capture the light waves leaving the patient’s retina.
“Essentially this optical table is a cross between a telescope, a microscope and a camera,” says Dubra. Though the construction doesn’t appear especially noteworthy, the images it produces of the surface of the retina are nothing short of astounding. Whereas in the past researchers struggled to pick out landmarks in what would look like a uniformly gray circle crisscrossed with blurry, hardly visible blood vessels, it’s now possible to clearly see individual red blood cells slowly pulsing their way, doubled over, through the tiniest retinal capillaries. Individual cone and rod cells seem to leap out at the viewer, and Dubra and his colleagues have even made progress toward identifying whether those cells are functional by, ironically, watching them twinkle like stars in response to flashes of colored light.
“Suddenly, it seems feasible to test a subset of cells in the retina, and maybe identify, for example, a handful of cells that are present but not functional,” says Dubra. “Medically this is potentially very important. Gene therapy approaches, for example, rely on the presence of nonfunctional cells that could receive a corrected version of a faulty gene.
“There are two major leaps we have wanted to make in our research,” he adds. “We want to go from looking at structures in the retina on a relatively macroscopic scale to a microscopic scale — visualizing individual rods and cones, capillaries and blood cells in real time in a living eye. We’re well on our way now, but there is still a fair amount of work to do. Secondly, and arguably more importantly, we’d like to find ways to monitor the function of these cells at a microscopic level. Maybe we can find a few thousand, or even a few hundred, cells that are not healthy. That may allow us to begin therapy before the patient experiences the ‘point of no return,’ or permanent, irreversible vision loss.”
Testing new instruments
Dubra has not forgotten his ultimate goal to help those suffering from vision loss. In June, he and his lab members moved into the just-completed Mary M. and Sash A. Spencer Center for Vision Research, next-door to Stanford’s Byers Eye Institute building.
“In the new Spencer Center, we will develop and test the new generation of adaptive optics instruments in labs immediately adjacent to the rooms where they will be used to examine and diagnose patients,” says Dubra. Currently instruments built by the Dubra lab are also being used, among other places, in the New York Eye and Ear Infirmary of Mount Sinai to study vascular diseases of the retina and at the University College London, the Medical College of Wisconsin and the University of Pennsylvania to identify good candidates for the world’s first gene therapy trials aimed at rescuing damaged cone cells in the retina.
“Now we can tell how many cone cells a patient has before they enroll in the trials,” says Dubra. “We can also follow patients over time to identify much more quickly those who might be benefiting from the treatment even before they experience functional changes in their vision.”
The instruments also allow researchers to monitor the progress of blinding diseases in real time, rather than relying on cadaver tissue donated by people who had already lost their sight. This is particularly important for the numerous conditions that manifest only in a small number of individuals, such as in 1 every 100,000.
“We now have the opportunity to start to really understand and monitor the pathophysiology of these blinding diseases,” says University College London’s Michaelides. “Alf has a rare ability to interact with both scientists and clinicians to develop the technology necessary to help us help patients.”
“I often think of that mom from my early days as a researcher in Rochester,” Dubra says. “I wish I could talk to her now. I could outline the concrete ways that our work is moving the field forward in ways that will directly benefit people like her son.”
