
Stroke
Treating blood clots in the brain goes from fast to faster to fastest
By the time the man arrives at Stanford Hospital’s emergency bay doors, paramedics have already called in vital information: He is unable to move his right arm and his speech is garbled, suggesting a stroke. His blood glucose is normal, ruling out hypoglycemia as the culprit.
As soon as the ambulance rear doors open, at 3:47 p.m., a clerk leans inside to record the man’s name, then runs back to the registration desk to enter his information into the system. A few yards beyond the ambulance bay a crowd of physicians, nurses and a pharmacist are waiting.
The paramedics lift the man (a composite Stanford stroke patient created for the scenario described here) onto a hospital gurney. With the press of a button, the gurney records the patient’s weight (let’s call him David Williams), and the crowd wheels him into the computed tomography room.
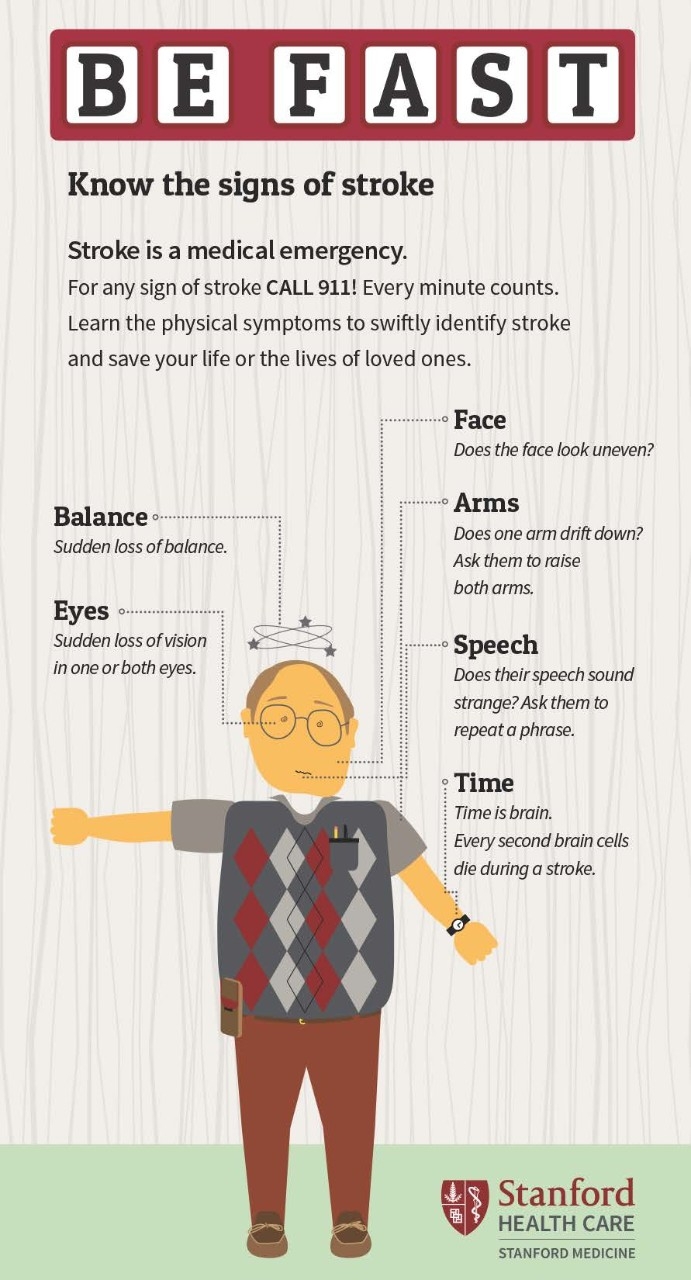
Signs of a stroke
How to tell if someone is suffering a stroke, and what to do about it.
They quickly transfer him onto the CT bed, positioning his head inside the doughnut-shaped scanner. One of the paramedics, meanwhile, calls out his medical information: “Right-side facial droop, aphasia. Age 82. Last OK was 2:30.”
While the scanner takes detailed X-ray images, the medical team stands behind a glass partition, eyes on computer screens. They are watching for telltale signs of bleeding in the brain, which would appear in the form of white, shapeless masses.
Once the scan is complete, as cross-sectioned images of Williams’ head flow onto the screens, nurses insert an intravenous line into his arm and draw his blood. Out in the hall, a pharmacist searches for Williams’ medical information in Stanford’s records.
“During a stroke, 1.9 million neurons die every minute. When we are able to administer tPA quickly, that translates into saved neurons, saved independence and saved health care costs.”
The physicians need to decide, quickly, if tissue plasminogen activator would help. The medication will dissolve a stroke-causing blood clot, but it will worsen and may provoke cerebral bleeding. If tPA is warranted, they must give it immediately, in the scanner room: Minutes saved in stroke treatment can make the difference between walking and not walking, living alone and relying on caregivers.
The pharmacist finds that Williams is not taking any medication nor does he have a medical condition that could lead to bleeding. The neurologist orders tPA, the pharmacist hands a nurse the correct dose in an IV bag and the nurse sets the pump to deliver the medication. A quality assurance nurse checks his watch: 4:02 p.m. Fifteen minutes have passed from the moment the ambulance bay doors opened until the tPA entered Williams’ vein.
“During a stroke, 1.9 million neurons die every minute,” said Nirali Vora, MD, an associate professor of neurology and a stroke specialist. “When we are able to administer tPA quickly, that translates into saved neurons, saved independence and saved health care costs.”

Seven years ago at Stanford Hospital, the average door-to-needle time — starting when a stroke patient arrives at the emergency department and ending when they receive tPA — was 66 minutes, typical for a U.S. hospital. Today, at Stanford, it’s 26 minutes, with an all-time record of nine. Shaving so much time from a process, in a department already primed for quick action, required months of research, years of changing work habits and a good dose of diplomacy.
Developing new stroke protocols
The rapid stroke protocol at the bustling emergency department got its start at Stanford’s Clinical Excellence Research Center. CERC’s office lies in the oak-studded hills about a mile south of the center of campus, reached by a winding, single-lane road.
CERC is the brainchild of Arnold Milstein, MD, an economics major who entered medical school and specialized in psychiatry and care quality before turning his attention to the rising cost of U.S. health care. Funded by grants and private foundation gifts, CERC generates research on lowering health care costs while preserving or improving quality.
Every year, CERC accepts and funds four to seven fellows, early career professionals with an interest in health care value. Most fellows work in the medical field, though some come from the business and engineering worlds. Split into two groups, they spend 11 months tackling two challenges that Milstein chooses. “I work backward,” Milstein said. “I ask, ‘Where is America spending the most on health care?’ Then I pick a plausible target.” CERC fellows have developed recommendations for such aspects of health care as outpatient surgery, prescription medication, spine pain treatment and ICU care.
During the second year of the program, 2012 to 2013, one of the teams took on stroke care, the leading cause of disability in the United States. The fellows started out “in a sort of innovation camp,” according to Waimei Amy Tai, MD, who was one of the stroke fellows and is now a neurologist at Christiana Care Health System in Delaware.
“I work backward. I ask, ‘Where is America spending the most on health care?’ Then I pick a plausible target.”
They learned about the economics of medicine as well as lean process management, a manufacturing approach that maximizes customer value by minimizing waste. They pored over the scientific literature on stroke care innovation and visited health care facilities to observe treatment protocols. They took a field trip to Hillsboro, Oregon, to learn how Intel reduces waste in its microchip fabrication plant.
Their research completed, the fellows devised three proposals to lower spending by improving stroke care: coaching patients to better manage their blood pressure, avoiding long hospitalizations for stroke patients whose symptoms disappear before or during emergency department visits, and sharply reducing door-to-needle times.
In the next step of CERC fellowships, the fellows pitch their proposals to health care organizations and share them at medical conferences, hoping to find buyers for their ideas. Virginia Mason Medical Center in Seattle and Allina Health in Minneapolis took on the second proposal, avoiding long hospitalizations. Kaiser Permanente’s Northern California hospitals adopted the third proposal, reducing door-to-needle times, as did Stanford Health Care.

Shaving off the minutes
Stanford’s new door-to-needle protocol was inspired by a stroke treatment innovation at Helsinki University Central Hospital; the CERC fellows uncovered it in a Scandinavian medical journal. In the Helsinki hospital, staff reduced their average time from nearly two hours to less than 20 minutes, largely by eliminating unnecessary steps and starting evaluations while stroke patients were traveling to the hospital.
But simply telling the staff at Stanford Hospital’s emergency department to follow the Finns wouldn’t bring lasting changes. “You have to understand how attached people are to their sense of mastery,” Milstein said. “They are grounded firmly in how they currently do their work.”
The task of reducing door-to-needle times fell, in part, to Tai, who stayed at Stanford for two years after the fellowship ended. Like Milstein, Tai was an economics major. “I’ve always had an interest in quality improvement,” she said. “I applied to CERC because I wanted to take a look at health care from a value perspective.”
Tai, Vora and other physicians, as well as nurses and CT technicians, began their project by observing. Whenever the charge nurse issued a stroke code — a text message alerting on-call nurses, pharmacists, registration clerks and physicians that a stroke patient is on the way — they watched.
They identified a few steps that were unnecessary, such as running an electrocardiogram and assigning a room, and eliminated them. They also realized that some steps, such as inserting an intravenous line and running lab work, could take place after the scan. They saved time by ensuring everyone on the stroke code team knew in advance the role they’d play in getting the patient to the CT scanner and, ultimately, treatment.
“There was a lot of resistance initially because we were changing people’s habits.”
Like actors rehearsing for a play, they ran mock stroke codes with one staff member playing patient and everyone else acting out their assigned roles. When they found snags, they fixed them and ran more mock stroke codes, shaving off minute after minute.
“There was a lot of resistance initially because we were changing people’s habits,” Tai said. She employed a host of management tactics, but perhaps her most effective tool was humility.
“At a meeting, I would suggest inserting the IV while we were waiting for CT scans, and no one would say anything,” she said. “Then I would email reference papers around, and someone at the next meeting would say, ‘Why can’t we insert the IV in the CT scanner?’ and I’d say, ‘That’s an awesome idea!’”
When Tai left Stanford in 2015, Vora took on the job of overseeing stroke care in the emergency department. At that time, stroke patients arriving by ambulance received speedy treatment, but those who showed up on their own were put through the old, slower process.
Like Tai, Vora spent a lot of time hanging out in the emergency department, waiting for potential stroke patients to walk in. When they did, she tried to blend into the background, timer in hand. Suspected stroke patients now have a bed reserved for them near the CT rooms — it signals that they need immediate testing — and triage nurses are empowered to call a stroke code. So are the security guards, who Vora ensured were trained to recognize a possible stroke. “Patients often tell the security staff their symptoms,” she noted.
A little competition also helped drive the numbers lower: The stroke team started issuing buttons that display the minutes it took from a patient’s arrival to the administration of tPA. If the door-to-needle time is impressive, under 30 minutes or so, stroke code team members pin them to their white coats and badge lanyards.
Continuing to improve
Eric Bernier, RN, was typing an email early this year when his cell phone flashed: “Stroke code adult: Emergency room ambulance bay ETA-10.” He put on his white coat and walked upstairs to the emergency department. As a quality director for Stanford Health Care, his job is to keep the door-to-CT and door-to-needle times low and to ensure that all the steps in the stroke protocol are followed. “I’m the grumpy guy in the basement who asks why things are taking so long,” he said.
On this day, he observed as the emergency crew ran through its well-practiced choreography and started the CT: It took just five minutes, one less than average. The process played out as it should, except, he noticed, an emergency technician failed to record the patient’s weight. He made a note to speak with her supervisor. “Every stroke code is an opportunity to find something to improve on,” he said.
Soon after the CT, the patient answered questions and was able to move her leg, so the neurology fellow on duty, Adam MacLellan, MD, decided against giving her tPA. “I’m more suspicious it’s a seizure,” he said. The lanyard holding MacLellan’s Stanford Hospital badge is covered in buttons with his door-to-needle minutes: 21, 25, 17.
Only about a third of stroke codes result in a stroke diagnosis — a migraine, low blood sodium, fainting, even reactions to Novocain from a dental procedure can look like a stroke. But because a stroke can be so devastating, Bernier said, “We’d rather activate way over. We say call often and call early” whenever a stroke is suspected.
And only about one-eighth of stroke codes end with tPA being administered. But the speedy system also helps patients with a stroke that tPA can’t treat: Quick diagnosis leads to rapid treatment — such as removing a clot with a device or repairing a damaged vessel — which means more brain tissue is protected.
If a door-to-tPA time is overly long, Bernier said, it’s usually because it took time to confirm information about the patient. Stroke patients often can’t speak, and family members or caregivers frequently don’t know what medications they’re taking. It can also take a while to determine when the stroke occurred; after 4½ hours, tPA is likely to cause more harm than good. In one case, the physicians determined the last time a patient was OK by reading a post on the patient’s Facebook page.
But if a patient’s record is readily available, the door-to-needle time can drop significantly: “When we had that nine-minute code, we had all the information on hand,” Bernier said. “Everything was in perfect alignment.”
A patient’s perspective
Malinda Mitchell, retired CEO of Stanford Health Care, was speaking with her mother, Rosina Might, in her kitchen when Might’s face started to droop. Mitchell, a former nurse, suspected a stroke and called 911. While she was on the phone, her mother collapsed, wouldn’t answer questions, and was unable to move one of her arms and one of her legs. An ambulance arrived in minutes.
By the time Mitchell and her sister, who was visiting along with their mother from Atlanta, made it to Stanford’s emergency department, Might was undergoing a CT scan. Seventeen minutes after her arrival, she received tPA — a record at the time, 2015.
“When we had that nine-minute code, we had all the information on hand. Everything was in perfect alignment.”
“The coordination and how synchronized they all were,” Mitchell said, “was really an amazing thing to experience from the patient side.”
Might, then 92, spent two days in the hospital and flew home two days later. “It was clearly a fairly massive stroke,” Mitchell said. “But the next morning she was talking in full sentences and moving her arm and leg.”
Might died last year at 95. Without effective stroke treatment, Mitchell said, her mother could have spent the last years of her life unable to speak, possibly paralyzed, relying on round-the-clock care.
Instead, Mitchell said, “She lived a very productive, active three years. It was as if nothing had happened.”
